a 59 year old male presented with a complex VHR via robot laparoscopy. He had a prior history of drug abuse, hepatitis C and a long smoking history resulting in mild undiagnosed and untreated COPD.
The patient was given a GETA anesthetic with sevoflurane, rocuronium, dilaudid, and low dose ketamine. During the anesthetic, his minute ventilation was unusually large for this 71 kg male. His peak airway pressures were also elevated despite no trendelenburg positioning requested from the surgeon. The procedure began at approximately 7:45am and closure was completed just prior to 5:00pm. Multiple ventilation manipulations were provided in an atttempt to improve ventilation, decrease airway pressures including driving pressure as well as minute ventilation.
In the October 2020 Journal Anesthesiology [1], An article on ventilation in obese patients undergoing laparoscopy surgery appeared. This article discussed a new paradigm emerging in ventilatory medicine to improve ventilation while reducing the incidence of ventilator induced lung injury (VILI). Dozens of studies showed reduced mortality in ICU patients who were ventilated due to ARDS when they were treated with low plateau pressure (Pplat) which often required reducing tidal volumes (Vt) to around 6 to 8 mL/kg and permissive hypercapnia. This has evolved over the years and there are now several studies indicating that the improvement in outcomes may be related more to reducing the driving pressure (Pdrive) rather than a purely low Vt permissive hypercapnea strategy.
It is noted that Transpulmonary pressure is the pressure felt by the lung tissue itself and therefore the main concern when attempting to limit or avoid VILI. It has been identified that during robotic surgery in particular, airway pressures generated when attempting to ventilate the patient are not similar to a patient who is undergoing non robotic surgery. In particular, the airway pressure measured by the ventilator is diverted from the lungs to the chest wall. This occurs because during robotic surgery, chest wall compliance can decrease by up to 300% while lung tissue compliance decreases by only 50%, and thus. To restate, higher chest wall stiffness results in a lower fraction of airway pressure distributed to the lungs during the Trendelenburg position and docked robot condition than after intubation. Measurements in non obese patients, after docking and insufflation of the abdomen, found that the fractional pressure presented to the lungs by mechanical ventilation is reduced (48% from 63% immediately after intubation). In the obese patient (BMI 30-40), the decrease is from 80% after intubation to 56% after docking. In essence, because the chest wall compliance decreases dramatically after docking the robot, the lungs are now "protected" or shielded to a degree from high "airway pressures". To illustrate, lets take an example patient with BMI of 40 whose plateau pressures immediately after intubation are 27 cmH2O. If 80% of this pressure is distributed to the lungs, they would be impacted by (0.8 x 27)= 21.6 cmH2O while the rest would be distributed to the chest wall. Now, after docking, and pneumoperitoneum has been established the Plat increases from 27 cmH2O to 35 cmH2O. If we now calculate the fractional pressure applied to the lungs we see that it is (0.56 x 35) = 19.6 cmH20. The other pressure is applied to the chest wall (35 cmH2O - 19.6 cmH2O)= 15.4 cmH2O. Obviously, these numbers are explanatory only to make a point. However, it is important to understand that this occurs due to the differential change in compliance of the chest wall (decreased by up to 300%) vs the decrease in compliance of the lungs (up to 50%).
Overzealous limitation of PEEP or tidal volume to maintain plateau pressures less than 28 to 30 cm H2O in such cases could expose patients to unnecessary hypoxemia, hypoventilation, and mechanical injury.
After the benefits of lower tidal volumes and permissive hypercapnea were realized, a large number of studies attempting to translate these results into clinical anesthesia were published. Unfortunately, the results were scattered with many studies unable to clearly show definite and meaningful benefits with "lung protective ventilation" strategies during routine clinical mechanical ventilation. In general, patients were divided into groups of high vs. low Vt (i.e. 10-12 ml/kg vs. 6-8 ml/kg) and groups of standard PEEP or no PEEP. The PEEP applied was usually standardized in the group that received PEEP anywhere from 2 up to 10 cmH20. Another recent trial found that PEEP of 12 cmH2O vs. 2 or less provided no benefit to patients undergoing open abdominal surgery. While there was no improvement in post op pulmonary complications (PPCs), the high PEEP group experienced more hemodynamic instability and required more fluid. This led many to recommend low PEEP. However, Tharp et al. [1], showed that individualizing applied PEEP, improves mechanical ventilation parameters. Tharp et al found that in patients with normal BMI, optimal PEEP was 9.7 cm H2O (+/- 3.7), whereas, for obese patients (BMI >= 40), optimal PEEP was 21.3 cmH2O (+/- 7.4). High PEEP has been shown beneficial in other studies of obese patients with ARDS, where PEEP as high as 20 cm H2O showed benefit[3]. The real takeaway from the Tharp paper [1], is the observed high variability in optimal PEEP between patients.
Post operative pulmonary complications and VILI can be understood by stress and strain placed on the alveoli. Excessive alveolar strain during ventilation may result in injury, and in predisposed patients will lead to post operative pulmonary complications (PPCs). Strain to the alveoli can be quantified and understood via the equation Vt/FRC ratios. Since the strain is equal to the ratio of change in volume to initial volume, understanding that if FRC drops in your patient as you anesthetize them, total alveolar strain will increase. As example, if you have a two patients both with Vt of 500ml but different FRCs, they will experience large differences in total alveolar strain during ventilation.
Patient 1: Vt=500mL and FRC 2000mL strain = 25%
Patient 2: Vt=500mL and FRC 500mL (due to ARDS) strain = 100% (four fold increase)
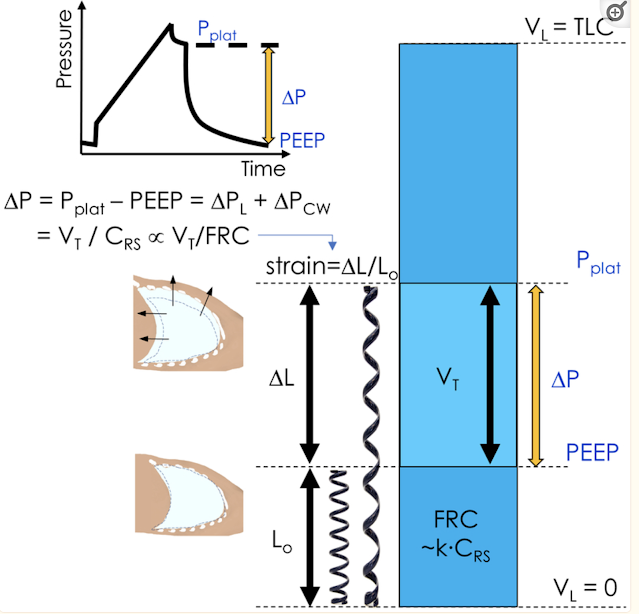
Intraop, we can't directly measure strain, although this variable is obviously incredibly important in causing lung injury if elevated. However, we can indirectly get clues as to the strain we are applying to the airways by measuring the driving pressure. Simply, Driving pressure (Pdrive) is the plateau pressure (Pplat) minus PEEP. Pplat is measured at the end of an inspiratory pause during volume controlled ventilation. The inspiratory pause is important as no flow can occur during measurement for accuracy. Fortunately, all modern anesthesia ventilators can apply this after each breath in order to measure Pplat. As we learn more about our ability to measure ventilation parameters and how to change those parameters to improve outcomes, anesthesiologists will find greater roles in controlling outcomes. Pdrive is a concept that is gaining greater traction. Essentially, Pdrive is expressed as the ratio between Vt and respiratory system compliance (Crs). Crs correlates closely with the aerated lung volume. Recent studies have demonstrated that Pdrive is a better indicator than purely Vt management to predict pulmonary outcomes. in 2015, a large analysis of patients with ARDS [4] was completed where it was shown that independent changes in Vt or PEEP were not independently associated with survival. However, Pdrive was associated independently with survival EVEN in patients receiving protective Pplat and Vt. In this study, the cut off point where risk was increased was Pdrive of 15 cmH2O. One year after the above was published a large meta analysis was completed looking at studies using "protective ventilation" to reduce post operative pulmonary complications [5]. They included data from 17 RCT with 2250 patients. A multivariate analysis suggested that Pdrive was associated with PPCs (there was a 13% increased probability of PPCs for every 1 cmH2O increase in Pdrive). There was no association at all with Vt or PEEP.
Unfortunately, Pdrive as a surrogate for acquiring measurement of transpulmonary pressure (what we are really after) can be unreliable in situations where Chest wall compliance is dramatically altered. This occurs as mentioned above during laparoscopy especially when robotic and in steep trendelenburg positioning. For example, increasing intraabdominal pressure increased Pplat by 50% of the applied intraabdominal pressure, but produced minimal change in transpulmonary pressure (Plung) in healthy lungs. In contrast, in the presence of lung injury, both Pdrive and Plung increased with increasing intra-abdominal pressure. In obese patients undergoing robotic laparoscopic surgeries, adequate mechanical ventilation may be difficult. In these situations there is a push to use esophageal manometry to directly measure pleural pressure which allows a direct measurement of transpulmonary pressure. Unfortunately, esophageal manometry is unavailable in routine clinical anesthesia. Therefore, given the tools at our disposal, how does one determine the "ideal" PEEP so as to decrease Pdrive when it becomes a challenge. As made clear above, routine application of 5 cmH2O of PEEP is likely not what any given patient will need. Previous studies have shown that "ideal" PEEP in obese patients ranged from 13 to 25 cmH2O. Tharp found using individualized PEEP titration using esophageal manometry that not all obese patients require higher PEEP settings. High PEEP can reduce venous return, right ventricular after load, cerebral perfusion pressure, and increase the potential for barotrauma and increased ICP. Therefore, much consideration should be given prior to simply increasing PEEP beyond 10 cmH2O when one encounters troublesome ventilation parameters. Finding "ideal" PEEP was highlighted by an article in the journal Anesthesiology [6], where it was demonstrated that when 'ideal' PEEP was identified using electrical impedance tomography intraoperative oxygenation, Pdrive, and post operative lung collapse were all improved. They also determined that ideal PEEP varied greatly between patients, and those receiving 'ideal' PEEP had no adverse affects. These authors were also able to demonstrate that applying a uniform level of PEEP to all patients can be problematic. During their recruitment process they were able to observe that a fixed PEEP of 6 cmH2O caused a wide range of lung collapse from 3 to 33% of the lung volume. At the other extreme, a fixed-PEEP of 16 cmH2O caused 5 to 52% of lung hyper distention. This study was also able to demonstrate a strong correlation between increasing BMI and higher ideal PEEP, but again, there was large variability. Tharp was [10] also able to demonstrate, that PEEP requirements also increase with the trendelburg position.
Unfortunately, the above technique of electrical impedance tomography is not available clinically. However, Park et al.[7] studied PEEP titration to Pdrive in an RCT of patients undergoing one lung ventilation for esophagectomy. One group received "protective" ventilation parameters by using 6 mL/kg of IBW Vt and PEEP of 5 cmH2O with recruitment maneuvers while the test group had their PEEP titrated. Starting at a PEEP of 2 cmH2O, they calculated Pdrive for the patient by using an inspiratory hold of 30% of inspiratory time to measure Pplat and then subtracted PEEP (Pdrive =Pplat-PEEP). After every change in PEEP, then allowed ten breath cycles to occur, and then used the Pplat of the last cycle for the measurement. After they tried PEEP 2 through 10 cmH2O, they used the PEEP at which the Pdrive was the lowest. PPCs were decreased from 12.2% in the protected ventilation group to 5.5% in the titration of Pdrive group which was statiscally significant (OR 0.4). A meta analysis of various set PEEP levels compared to individualized PEEP found that individualized PEEP was superior to set PEEP values (from low to high) in terms of oxygenation and lung compliance. In another RCT [8] in elderly patients undergoing laparoscopic surgery, titration of best PEEP from 4 to 10 cmH2O was compared to a convention group (Vt 10 ml/kg no PEEP) and a protective ventilation group (Vt ml/kg IBW and PEEP of 6 cmH2O). The CV and PV groups had similar post op pulmonary profiles vs much improved profiles in patients whose PEEP was titrated to the lowest Pdrive. Similar results were found in patients having a lapx chole [9].
Unfortunately, while it seems clear that reducing Pdrive and titrating PEEP to the lowest Pdrive in patients improve pulmonary profiles, several questions remain: In which patients should we use these procedures, which types of surgeries, what PEEP level should be tried, what Pdrive is too high, and how often should we reverify ideal PEEP Intraoperatively?
My patient had high Peak airway pressures as well as high Pdrive. I tried to titrate my PEEP higher and this did help reduce Pdrive, but it remained around 14 to 16 cmH2O with even though PEEP was set to 12 to 14 cmH2O.
Very recently a large retrospective study was published in Anesthesiology [10] where much of the concepts discussed above were established further. Importantly, the study authors concluded that mechanical power is independently associated with increased post op pulmonary complications (PPCs). Importantly, in this study, PEEP was not associated with PPCs and decreased Vt was associated with increased PPCs. The authors provided two explanations for why a presumably protective strategy (low Vt) would be associated with increased PPCs. 1) it may be that patients at higher risk were set to lower Vt ventilation by clinicians than normal (although this was controlled for using statistical analysis) and 2) decreased Vt caused increased PPC by allowing atelectesis to develop that was not appropriately offset with appropriate levels of PEEP with recruitment maneuvers. Mechanical power is defined as the energy transferred to the respiratory system and the lung during mechanical ventilation in J·min−1. This concept has the advantage of encompassing all ventilation parameters previously considered in protective ventilation and also takes respiratory rate (RR) into account. To determine mechanical power there are several equations, one of which is:
MP (J/min) = 0.098 × RR × Vt × (PEEP + ½[Pplat − PEEP] + [Ppeak − Pplat]).
The important feature to note is that respiratory rate (RR) is directly correlated with mechanical power. Therefore, from this equation we can see that when a clinician decreases Vt to protect the lungs, they typically increase RR to maintain adequate ventilation. From the equation, this change will keep mechanical power unchanged. It is important to note that the concept of mechanical power was previously documented to be associated with increased rates of respiratory failure after non cardiac general anesthesia [11]. This group noted the following in their paper, "In an exploratory, post hoc defined analysis, we found that an intraoperative threshold increase of mechanical power by at least 2 J/min, which was driven by higher driving pressures and respiratory rates, was associated with 28% greater odds of developing postoperative respiratory failure."
In summary, the current strategy of using 6 mL/kg for Vt and setting the PEEP to 5 cmH20 for all patients undergoing general anesthesia is not likely to reduce PPCs. A more nuanced approach, where the driving pressure (Pdrive) and the overall stress applied to the pulmonary system (Mechanical power) is called for in higher risk patients. Reducing Mechanical power can be achieved by optimizing PEEP to the patient, maintaining lower respiratory rates and taking note of the driving pressure which should be lowered.
1. Tharp WG et al. Anesthesiology V133, issue 4, 2020
2. Bao X, Vidal Melo M. Anesthesiology V133, issue4, 2020
3. Florio G, Ferrari M, Bittner EA, De Santis Santiago R, Pirrone M, Fumagalli J, Teggia Droghi M, Mietto C, Pinciroli R, Berg S, Bagchi A, Shelton K, Kuo A, Lai Y, Sonny A, Lai P, Hibbert K, Kwo J, Pino RM, Wiener-Kronish J, Amato MBP, Arora P, Kacmarek RM, Berra L; i Crit Care. 2020 Jan 15;24(1):4.
4. Amato MB, Meade MO, Slutsky AS, Brochard L, Costa EL, Schoenfeld DA, Stewart TE, Briel M, Talmor D, Mercat A, Richard JC, Carvalho CR, Brower RG. N Engl J Med. 2015 Feb 19;372(8):747-55.
5. Neto AS, Hemmes SN, Barbas CS, Beiderlinden M, Fernandez-Bustamante A, Futier E, Gajic O, El-Tahan MR, Ghamdi AA, Gunay E, Jaber S, Kokulu S, Kozian A, Licker M, Lin WQ, Maslow AD, Memtsoudis SG, Reis Miranda D, Moine P, Ng T, Paparella D, Ranieri VM, Scavonetto F, Schilling T, Selmo G, Severgnini P, Sprung J, Sundar S, Talmor D, Treschan T, et al.: . LancetRespiratory Med 2016; 4:272–80
6. Pereira S, Tucci M, Morais C, Simons C, Tonelotto B, Pompeo M, Kay F, Pelosi P, Vieira J, Amato M. Anesthesiology December 2018, Vol. 129, 1070–1081.
7. Park et al. Anesthesiology. March 2019, Vol. 130, issue 3
8. Xu Q BMC Anesthesiology. 2022; 22:72.
9. D’Antini D, Rauseo M, Grasso S, et al. Physiological effects of the open lung approach during laparoscopic cholecystectomy: focus on driving pressure. Minerva Anestesiol. 2018;84(2):159–67.
10. Bertrand ElefterionCedric CireneiEric KipnisEmeline CailliauAmélie BruandetBenoit TavernierAntoine LamerGilles Lebuffe; Intraoperative Mechanical Power and Postoperative Pulmonary Complications in Noncardiothoracic Elective Surgery Patients: A 10-Year Retrospective Cohort Study. Anesthesiology 2024; 140:399–408 doi:
11. Santer P, Wachtendorf LJ, Suleiman A, Houle TT, Fassbender P, Costa EL, Talmor D, Eikermann M, Baedorf-Kassis E, Schaefer MS. Mechanical Power during General Anesthesia and Postoperative Respiratory Failure: A Multicenter Retrospective Cohort Study. Anesthesiology. 2022 Jul 1;137(1):41-54. doi: 10.1097/ALN.0000000000004256. PMID: 35475882.

No comments:
Post a Comment